
Facebook
Twitter
LinkedIn
When Samantha stepped into her new role as Chief Operating Officer of a major health system, she was brimming with confidence. Her CV sparkled: decades of operational excellence, accolades for turnaround results, and a reputation for decisive leadership. She’d led complex divisions before. What could possibly go wrong this time?By month six however, the energy had shifted. Meetings were tense, trusted partners seemed distant, and strategic initiatives were slowing rather than accelerating. By the end of year one, her board was questioning whether she was the “right fit”.
Samantha’s story isn’t an outlier. In fact, research shows that between 40% and 50% of senior leaders fail within their first 18 months, not because they lack intelligence or dedication, but because they misread what success in transition actually requires.
In healthcare, the stakes are even higher: failure doesn’t just affect financial performance, it affects patient safety, workforce stability, and community trust.
The truth is that most senior leaders don’t fail because they lack competence. They fail because they misunderstand what the first year is really for. This is not a story about capability. It is a story about transition. And healthcare makes these transitions uniquely complex.
The First Year Isn’t a Trial. It’s an Investment.
Healthcare organisations often hire senior leaders with an implicit expectation: deliver early wins, demonstrate authority, move decisively. New executives absorb that pressure quickly. They know boards are watching. They know staff are evaluating them. They know performance metrics won’t pause while they “settle in.”
So they sprint.
But healthcare systems are not blank canvases. They are dense ecosystems layered with professional identities, informal power structures, historical tensions, funding constraints, and clinical cultures that have evolved over decades.
When leaders move too fast without understanding this ecology, they don’t accelerate progress. They activate resistance. Early action without contextual insight quietly erode credibility. In hospitals especially, where trust and professional respect underpin everything from theatre scheduling to incident reporting, credibility is the real currency.
The first year is not about proving your brilliance. It’s about building the foundations that will allow that brilliance to gradually land.
Listening Is Not Passive, it’s Strategic.
Healthcare leaders often come from high-performance backgrounds where decisiveness is rewarded. But in a new system, decisiveness without deep listening can be misinterpreted as disregard.
To be effective, first-year leaders must do something counter-intuitive: they must slow themselves down.
They must:
- Conduct structured listening tours across clinical and non-clinical teams.
- Ask the same questions repeatedly to identify pattern themes.
- Observe how decisions are actually made, not how governance charts suggest they are made.
- Map informal influencers alongside formal reporting lines.
In healthcare, power is rarely linear. A respected senior nurse unit manager may hold more operational influence than a titled executive. A long-tenured specialist may shape cultural norms far beyond their clinical remit.
Listening is not about being agreeable. It is about building an accurate mental model of the system. And in complex adaptive systems like health services, an inaccurate model leads to flawed interventions.
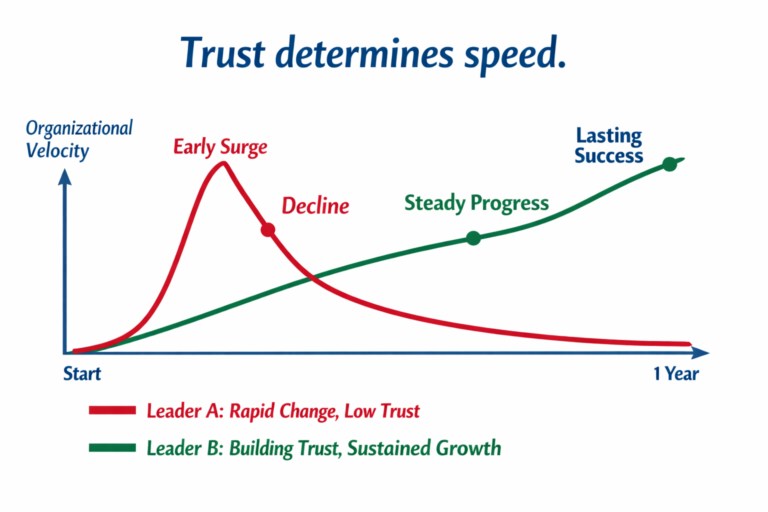
Trust Determines Speed
One of the most misunderstood aspects of leadership transition is velocity.
New executives often try to move quickly to demonstrate value. But in healthcare, speed is not determined by authority. It is determined by trust. When clinicians believe a leader understands their reality, initiatives accelerate. When they suspect misunderstanding, everything slows: approvals take longer, committees multiply, objections surface late.
Trust does not transfer with a CV. It must be built. Deliberately.
That means:
- Demonstrating clinical curiosity, not just operational urgency.
- Explaining the “why” behind decisions in language that resonates with different professional groups.
- Following through on small commitments consistently.
- Admitting what you don’t yet know.
Research in emotional intelligence consistently links self-awareness and empathy to team performance. In healthcare environments, where burnout is high and psychological safety is fragile, relational competence is essential. It is operationally decisive.
Trust is what converts authority into influence.
The Politics of Healthcare Are Structural, Not Personal
Many senior leaders privately confess they were unprepared for the political dimensions of their new role. Healthcare politics are not about ego, they are structural. Ignoring politics does not make them disappear. It simply means you are navigating without a map.
Sophisticated leaders approach politics somewhat more analytically. They identify:
- Who influences capital allocation decisions,
- Which peer alliances unlock cross-functional change,
- Where legacy loyalties may resist reform, and
- How board dynamics shape executive authority.
This is not manipulation. It’s systems literacy. In healthcare, where multidisciplinary collaboration determines patient outcomes, understanding political currents is part of responsible leadership.
Healthcare is particularly unforgiving because leaders must navigate layered governance: board oversight, clinical advisory structures, accreditation bodies, government stakeholders, insurers, and community expectations. Without structured transition support, even highly experienced leaders are forced to reverse-engineer success criteria while under scrutiny. That is a design flaw, not a personal one.
What a Strong First Year Actually Looks Like
When we study successful healthcare transitions, a different pattern emerges.
1. They slow down. Deliberately. Not to hesitate, but to diagnose. They treat the first 90–120 days as discovery. They test assumptions before formalising strategy.
2. They build three intentional networks.
Operational networks –the people who execute daily work,
Developmental networks –the mentors, peers, or advisors who provide perspective, and
Strategic networks -the individuals who influence capital, policy, or culture at scale.
In healthcare, neglecting any one of these weakens momentum.
3. They deliver one visible, aligned win.
Not a sweeping transformation. A well-chosen initiative that signals: “I understand this organisation, and I can work within it.” This builds belief.
4. They seek structured support.
Leaders who engage in executive coaching, formal assimilation processes, or board alignment conversations significantly increase their probability of sustained performance. Transition is not a test of independence. It is a test of adaptability.
The Deeper Issue: Identity Shift
There is an often-unspoken element to first-year failure -identity.
Many leaders are promoted because of what made them successful in their previous role -operational sharpness, clinical excellence, technical expertise.
But senior executive roles require a different orientation:
- From solving problems to shaping context,
- From controlling outputs to influencing systems, and
- From personal credibility to distributed trust.
If that identity shift does not occur, friction follows.
Healthcare amplifies this challenge because professional identity is deeply embedded. A former surgeon CEO must evolve beyond surgical thinking. A former nurse executive must lead beyond nursing paradigms. The leaders who thrive are those who consciously recalibrate how they see themselves, and how they create value.
Changing the Story
Samantha eventually found her rhythm. She recalibrated her approach, rebuilt alliances, and shifted from acceleration to alignment. But it cost political capital and emotional energy that could have been preserved.
Her story is not about failure.
It is about preventable friction.
For healthcare organisations, the lesson is clear:
- Treat executive transition as a strategic process, not an administrative event.
- Define what success in year one truly means.
- Invest in structured onboarding and coaching.
- Align boards and executives on pace and priorities early.
For healthcare leaders stepping into new roles:
- Resist the urge to prove.
- Diagnose before you prescribe.
- Build trust as intentionally as you build strategy.
- Understand that influence precedes impact.
Healthcare does not need more heroic first years. It needs wiser ones.
Because in a system already under strain -workforce fatigue, funding pressures, rising complexity, leadership instability is a risk we can no longer afford.
The first year is not about demonstrating power. It’s about building the relational and systemic foundations that allow meaningful, sustained impact to follow. And that is work that is worth doing well.
At the Australian Institute of Healthcare Executives, we work with senior clinicians and executives navigating exactly these transitions. Equipping them with the practical tools, strategic insight, and peer networks needed to lead complex health systems with confidence.
If you are stepping into a new role, or preparing for one, don’t leave your first year to chance.
Explore AIHE’s leadership courses and transition programs and invest in the kind of leadership that endures.
Because your first year should be the beginning of impact, not the start of recovery.

